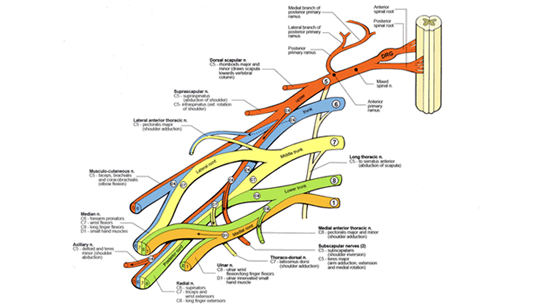
Plexus Injury with Neuroma
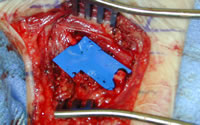
Plexus after Neuroma Removal
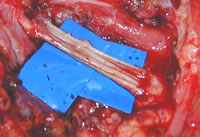
Nerve Grafting of Plexus
|
If
your child has weakness of shoulder, elbow, and/ or
hand by the age of 3 to 4 months, we strongly
recommend consultation with a surgical specialist with
extensive experience in obstetric brachial plexus injury.
If your child has no movement in any part of the arm by 3 months, we strongly recommend surgery at or before 3 months.
We have found this series
of steps to offer optimal results. The specifics
of application to each child is highly individual,
however, and of course other centers may have different
management protocols.
EMG's are ideally done
at 4 to 6 weeks of age to set a baseline for further
evaluation in the future. Similarly, an MRI
around that time can be done to determine whether
root avulsion (tearing of the roots from the spinal
cord) is present, although this test overall is less
important than a good EMG examination. The EMG should
then be repeated around 3 to 4 months of age to see
if improvement has occurred electrically, and to correlate
with the physical examination. Generally speaking,
if there is not full movement of all elements of the
arm (shoulder, elbow, hand) by 3 to 4 months, serious
consideration for operative exploration should be
initiated. If there is no elbow flexion by 6 months
of age, surgery is definitely recommended.
|