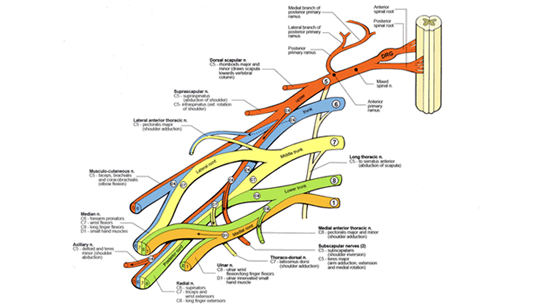
The most commonly injured elements of the brachial plexus in children are the upper roots. These injuries often lead to loss of abduction and external rotation of the shoulder due to deltoid, supraspinatus, infraspinatus and teres minor denervation. This results in a muscle imbalance that eventually causes contractures to develop about the shoulder joint. The Mod Quad surgery has been used in the treatment of these contractures with great success in the restoration of shoulder abduction.
However, the internal rotation posture in certain cases may have an additional component of bony rotation. This has significant functional consequences including limb shortening, loss of supination, winging of the scapula and lateral angulation of the elbow. Traditionally, the approach to this problem has been the use of derotational humeral osteotomy to neutralize the hand and forearm. This approach attempts to restore the arm to a neutral position and often does do so. It does not address the primary cause of internal rotation, so further management may be necessary.
Based on 3D CAT scans, it is apparent that the internal rotation of the arm associated with obstetrical brachial plexus injury is often related to a change in the spatial relationship of the scapula and clavicle. The elevation and forward rotation of the scapula causes positional changes in the acromio-clavicular (AC) joint.
The bony changes are collectively known as a SHEAR deformity (Scapular Hypoplasia, Elevation and Rotation). There are 5 grades (0 through 4). As a result, internal rotation posture of the arm is inevitable with
attendant functional and visible consequences. Physical therapy cannot significantly improve the appearance or function of the severely elevated scapula (Chung et al., 1975).
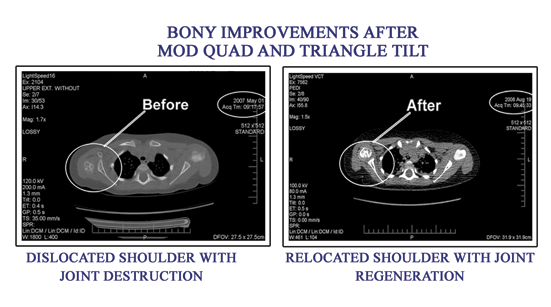
The Triangle Tilt surgical procedure combined with capsulodesis restores the arm to a more natural position by addressing the primary issue of scapular elevation. The clavicle and acromion are repositioned in a controlled fashion and allowed to re-align and interlock naturally, effectively restoring the spatial relationship of the clavicle and scapula (tilting the triangle). A posterior gleno-humeral capsulodesis is also performed at this time, to tighten the laxity of the shoulder that has been created by the malpositioned humeral head.
A 'SARO' splint ( Click here to see photos on the SARO splint ) is worn for a period of six weeks full time (24/7) followed upto one year or more at night after Triangle Tilt surgery to allow for the newly tilted triangle to heal and strengthen. A direct consequence of this intervention is correction of the internal rotation deformity and functional improvements in supination and hand-to-mouth movements. Additionally, the length of the arm is significantly improved, because of the repositioning of the gleno-humeral joint and better elbow extension. Therefore, the Triangle Tilt is an effective improvement on traditional surgical methods.