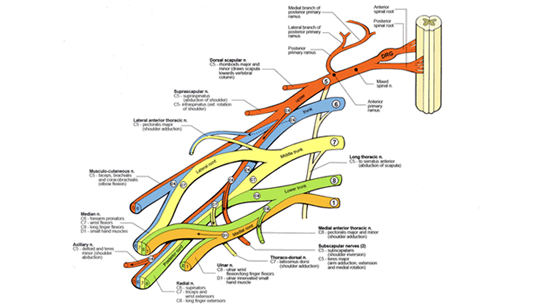
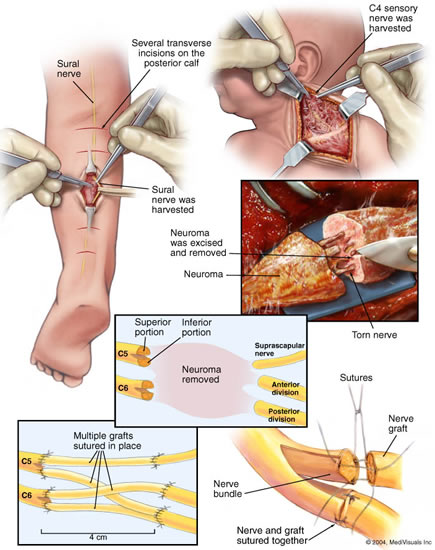
Brachial plexus anatomy is complex, but can be described in terms of basic function. The brachial plexus is derived from 5 "roots" or spinal nerves that exit the spinal cord in the neck. The nerves then pass through the axilla or armpit behind the collarbone (clavicle), and split into the final nerve branches that supply the muscles and skin of the shoulder, arm, elbow and hand.
The roots are named for the level of spinal cord that they exit. The upper roots (C5 and C6) exit from the cervical (meaning "neck") 5th and 6th vertebrae. The middle root (C7) exits above the 7th cervical vertebrae, and the lower roots exit from C8 (below the 7th cervical vertebra) and T1 (below the 1st thoracic vertebra). The upper roots supply upper structures (C5 to shoulder, C6 and C7 to elbow), and the lower roots supply the forearm and hand.
|