|
To date, Dr. Nath has performed secondary surgeries on over thousands of children and adults.
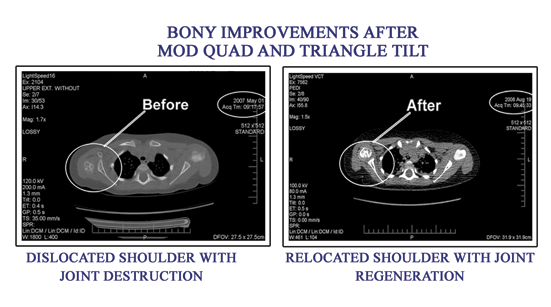
Secondary Surgery in Children with Brachial Plexus Injury (Mod Quad Operation): This does not mean that the primary surgery did not work. It describes another type of surgery later in time used to correct muscle imbalances.
The situation of muscle imbalance is very common among patients with Erb's palsy and with other brachial plexus injuries. In our experience the majority of children whose injury does not resolve completely by 3 to 4 months of age will end up with a specific series of arm restrictions caused by a muscle imbalance between injured and uninjured muscles.
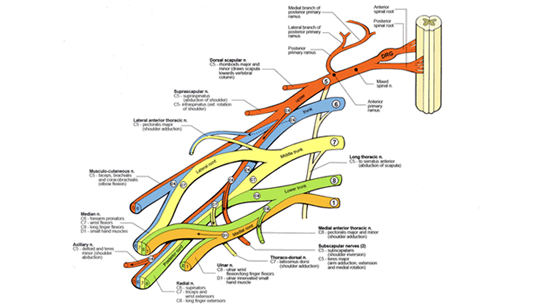
Among the muscles injured in Erb's are the abductors of the shoulder (that lift the arm over the head), as well as the external rotators (that help to turn the upper arm outward and to open the palm of the hand).
At the same time, the internal rotators (muscles that turn the arm and palm inward) and adductors (muscles that pull the arm to the side) of the arm are not involved in the injury because they are supplied by the lower roots of the plexus.
Therefore, these strong muscles overpower the weak muscles and over time the child cannot lift the arm over the head or turn the palm out, because of the muscle imbalance. |