|
OBPI Case Studies
Case Study, Obstetric Brachial Plexus
Injury
The patient is a full-term male child
with a birth weight of 8 pounds 11 ounces, born in New York
state. He was diagnosed with a shoulder dystocia during
the birth process, and was delivered after 12 hours of labor
with the use of a vacuum extractor. The child was noted
to be extensively ecchymotic in the area of the right shoulder
and body and with a cephalohematoma.
In the immediate postnatal period, the
baby was noted to have a flaccid right upper extremity and
torticollis. The affected arm was noted to be in an internally
rotated position at the shoulder with pronation at the wrist
and cupping of the fingers. X- rays of both clavicles and
humerus bones were obtained and found to be negative. A
consult with the physical therapy department was obtained
and gentle range of motion therapy instituted and taught
to the parents. The remainder of the hospital course was
unremarkable, and the child was discharged home in stable
condition. Followup appointments were made with pediatrics,
obstetrics, and the physical therapy department. Specialist
consultation with a local pediatric neurologist was arranged
at the age of 3 weeks.
By the age of three weeks, the child
had regained flexion of the fingers and wrist, to grade
3+ out of 5 on the British Motor Grading system. The remainder
of the extremity was essentially 0/5, with patchy sensibility,
although better in the hand than the shoulder area. Regular
visits to pediatric occupational therapy were instituted
at two to three times per week. The parents performed range
of motion and sensory rehabilitation training several times
each day as instructed by their occupational therapist.
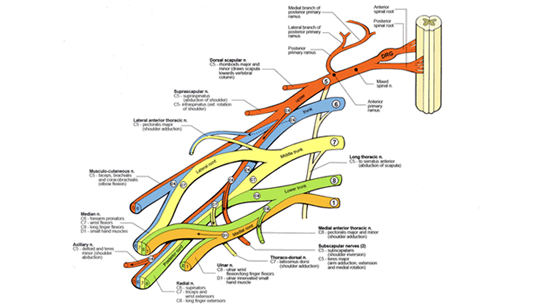
An electromyogram (EMG) of the upper extremity at 5 weeks
of age was consistent with a severe injury to the C5 and
C6 nerve roots with additional injury to C7 and partial
injury of the C8 and T1 roots.
At age three months, the baby was noted
to have improving triceps and wrist and finger extension
strength, to grade 3/ 5. The thumb remained tucked into
the palm but less tightly than at birth. A repeat EMG revealed
no improvement in the C5 and C6 distribution of the extremity,
but increasing motor units in the triceps, forearm and hand.
Because of the continuing deficits and positional abnormalities
as well as the static EMG findings in C5 and C6, the patient
was referred to the Brachial Plexus Clinic at Texas Children's
Hospital, the largest such clinic in the world.
A videotape of the child's arm and hand
movements while in the upright position was obtained and
mailed to the TCH Brachial Plexus Clinic. The video was
reviewed by a multidisciplinary team and based on clear
lack of antigravity function in the shoulder and biceps,
the child was scheduled for surgical intervention at 6 months
of age.
The child and his parents traveled to
Houston and were evaluated by the Brachial Plexus team the
day prior to the planned surgery. The child was confirmed
to have probable ruptures of the upper roots of the brachial
plexus and taken to surgery the following day. A team of
pediatric neurosurgeons and microsurgeons then reconstructed
the injury of the brachial plexus which was found to have
a complete rupture of the C5 and C6 nerve roots at the level
of the upper trunk. Nerve graft was taken from the ankle
area and used to reconstruct the torn nerves after removal
of scar tissue within the brachial plexus. Following a 4
hour surgery, the child was recovered in the hospital for
2 nights then discharged home with appropriate instructions.
A light sling was applied and range of motion therapy started
the day after surgery. Formal return to occupational therapy
began 3 weeks after surgery, although the parents performed
gentle ROM for those 3 weeks at home.
Over the course of the succeeding 3 months,
the child slowly improved in muscle tone of the arm with
steadily improving triceps and hand strength. Five months
after surgery, the child had for the first time exhibited
antigravity biceps movements sufficient to bring the hand
to the mouth, although with weak supination and a continued
tendency toward internal rotation at the shoulder. Shoulder
abduction was restricted to about 60 degrees with poor external
rotation. A videotape was at this time was evaluated by
the clinic surgical team and the movement pattern confirmed
as indicating the presence of contractures in the axilla
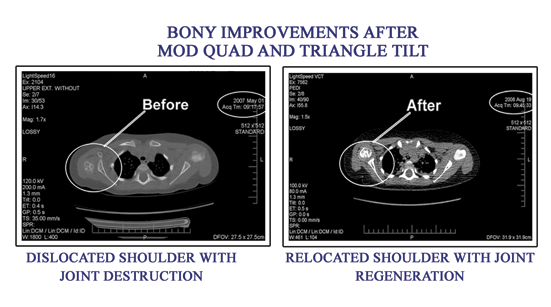
and chest. Upright xrays of the injured shoulder showed
significant deformity of the glenohumeral joint, with a
shallow glenoid fossa, hypoplastic humeral head, osteopenic
and thin humerus, and a high- riding and dysplastic scapula.
A posterior dislocation of the shoulder was diagnosed, due
to bony developmental abnormalities and muscle contractures.
The child was scheduled for Mod Quad surgery.
The Mod Quad surgery was performed by
a microsurgeon when the child was 12 months of age. The
tendon transfers, nerve decompressions and contracture releases
were performed through an axillary incision and the child
was placed in a statue of liberty splint for 3 weeks. Daily
ROM of the shoulder, elbow and hand joints was performed
each day by the parents for 30 minutes during the first
3 weeks. The splint was worn only at night for the next
3 weeks. Upon institution of formal therapy 6 weeks after
surgery the patient was noted to have gained significant
movement in active abduction, from 60 degrees to 150 degrees,
and in active external rotation from 0 degrees to 40 degrees.
Contracture tightness was resolved and virtually normal
passive ROM was seen.
Although active ROM and functional movements
increased 3-fold as a result of the Mod Quad surgery, an
internal rotation posture of the arm remained at rest. Therapy
continued 2-3 times per week, with the addition of Therapeutic
Electrical Stimulation (TES) at night. By the age of 2 years,
arm position was not improved and shoulder dislocation as
evidenced by continued internal rotation and lack of supination
continued. A biceps tendon contracture with a fixed elbow
flexion posture of 30 degrees was noted. The affected arm
was measured as 5 centimeters shorter than the uninjured
side.
The child was scheduled for anterior
shoulder capsule release and posterior capsulodesis surgery
to tighten and improve shoulder position. At the same time,
a lengthening of the biceps tendon to correct the elbow
flexion contracture was also performed. Following this surgery,
the child was in an external rotation splint for 8 weeks,
at which time therapy was resumed. The arm and shoulder
position were now noted to be normalized and supination
improved. Elbow position was neutral at 0 degrees. Arm length
was equal.
The child continued 2 to 3 times weekly
supervised therapy, through age 18 years, by which time
growth and development were essentially complete. Therapy
was reduced to once monthly for the next 7 years although
daily home stretching and strengthening exercises were taught.
For the remainder of adult life, therapy was maintained
at once each 3 to 4 months with daily home exercises. Yearly
consultation with a rehabilitation physician and the brachial
plexus clinic were maintained. At age 35 years, the patient
underwent carpal tunnel and ulnar nerve decompression and
transposition for documented nerve impingement. At age 45,
the patient had the same surgical procedures on the uninjured
side as a result of overuse syndrome. The patient had symptoms
of arthritis of the shoulder joint and fingers at age 50,
with chronic pain treated with nonsteroidal medications.
The patient was employed as an office manager and took early
disability retirement from work due to loss of work time
for pain management and therapy.
|
Contact US
|